Message intended for Healthcare Professionals Only
The history of synthetic materials started in the early 1900’s, when D.E. Robertson assayed a piece of cat bone and a piece of human bone for grafting into dogs. A microscopic analysis of implanted graft after 20 days showed that the space between the graft and the living bone was filled with new cancellous bone. This early work laid the foundation for the development of bone grafts.
First-generation bone grafts were developed in the latter half of the 20th century, and were shown to have remarkable mechanical properties, but no resorbable or bioactive properties.
Second-generation bone grafts were at least bio-resorbable or bioactive and did not need to be replaced. These second-generation grafts were composed of calcium phosphates (especially hydroxyapatite and tricalcium phosphate), bioglasses, alumina, zirconia, etc.
Third-generation bone grafts have been developed as bio-resorbable and bioactive materials with superior properties, strongly influenced by the nature of their components, their composition and the morphology. Third-generation bonegrafting biomaterials include (nano)hydroxyapatite/collagen, (nano)hydroxyapatite/collagen/hyaluronic acid, hydroxyapatite/poly-L-lactic acid, etc.
Fourth-generation bone graft biomaterials have been developed with features similar to those in the former generation, but with an improvement in the presence of bony cells, growth factors, bone morphogenetic proteins, etc.
One of the most important features of these new bone grafts is osteointegration, which is strictly related to the degree of porosity and the pore size of the scaffold.
Stoichiometric HA (Ca/P ratio = 1.67) is a mineral composed of calcium ions, phosphate ions, and hydroxyl groups. Given its close similarity to the mineralized phase of bone, HA shows high biomimetic properties, osteoconductive potential and excellent biocompatibility.
The porous architecture of the HA substratum, with its macropore network and its micropore interconnections, induces rapid vascular and mesenchymal invasion and provides a specific cell flow. These cells can attach, proliferate, and finally differentiate into functional osteoblasts. The osteoconductive property of HA has made this material of particular interest, since it can sustain new bone formation independent of the implantation site.
Ion substitution enhances HA instability and biological activity, promoting rapid cell-mediated material resorption, new bone formation and remodeling.33 As such, the design and development of a new generation of synthetic resorbable apatite substitutes has been stimulated to mimic some properties (chemical composition and three dimensional architecture) of the biological phase to overcome most of the limitations typical of stoichiometric HA implants.
Magnesium is one of the most important bivalent ions associated with biological apatite, since it is one of the most abundant minerals in the human body and approximately 50% of Mg2+ is naturally present in bone tissue. Mg2+ enables the HA crystal cell structure to become unstable and more biologically active, promoting rapid cell-mediated material resorption, new bone formation and remodeling by cross-talking with progenitor cells at the molecular level.
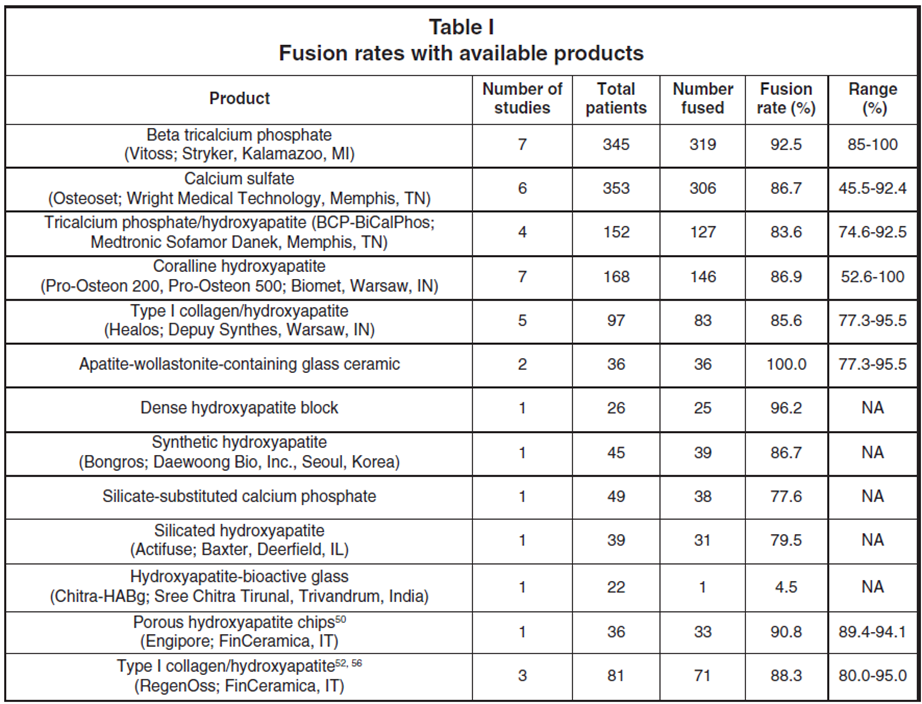
“Cumulative data with the different materials used in spinal fusion are summarized in Table I”
From Discussion and Conclusion
“the overall results demonstrated that fusion rates and functional outcomes were comparable for the considered bone graft extenders and the iliac crest bone graft group, confirming the safety and efficacy of these materials in spinal fusion procedures.
Among all of the biomaterials available, hydroxyapatite in particular is recommended as a bone graft substitute that closely resembles human bone, when combined with rigid internal fixation for necessary support.”
“A growing body of research on the topic suggests that bone graft biomaterials are safe and effective in spinal fusion procedures compared to iliac crest bone graft.
Among them, hydroxyapatite is recommended as a bone graft substitute when combined with rigid internal fixation for necessary support.”
“In conclusion, the use of ceramic derivatives as bone graft extenders is recommended to promote fusion in spinal instrumented fixation”
“Critical Evaluation of the Scientific Literature Concerning Bone Graft Alternatives in Spinal Surgery and Focus on Bioceramics” published on https://pubmed.ncbi.nlm.nih.gov/35738571/
Neuro and Spine Surgery SURGICAL TECHNOLOGY INTERNATIONAL Volume 41


